

Diagnosing keratoconus
Your ophthalmologist may use a number of tools to make a diagnosis of keratoconus, including:
- A slit lamp, which combines an intense light source with a microscope to examine your eyes
- A keratometer to measure the curvature of the cornea
- Corneal topography, which creates a 3D model of the cornea to detect any subtle changes.
Treating keratoconus
In the early stages of keratoconus, the only treatment required may be prescription glasses to correct your vision. Unfortunately, this is a progressive condition so your vision will eventually deteriorate, sometimes quite rapidly.
Below are some of the other keratoconus treatments your ophthalmologist may recommend.
Contact lenses
Rigid (hard) or hybrid contact lenses may be prescribed and are particularly effective in treating keratoconus for a period of time. These are made from a special material that allows the contact lens to mask the abnormal shape of the cornea and improve vision. However, contact lenses do not stop the condition from progressing and will eventually become ineffective.1
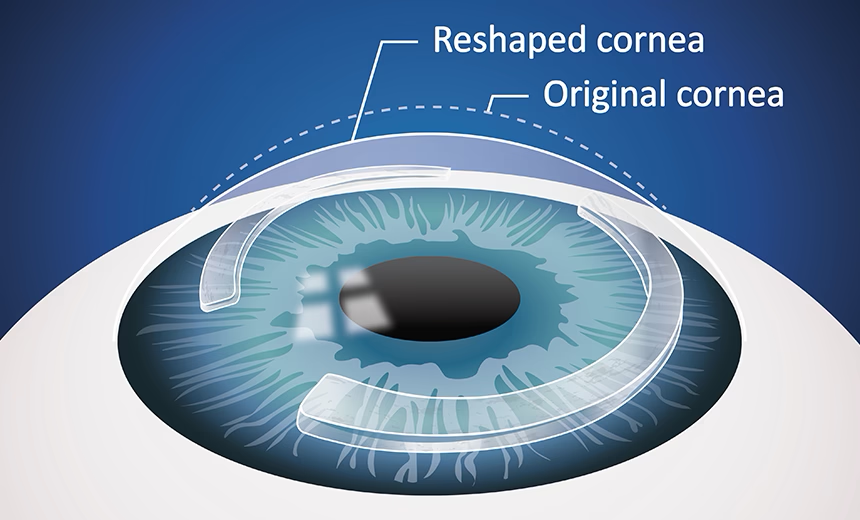
Corneal ring segments
Corneal ring segments are a surgical option for keratoconus treatment, aimed at correcting the irregular astigmatism and refractive errors caused by this progressive eye condition. This type of keratoconus surgery traditionally involved the insertion of clear plastic segments to reshape the cornea to improve vision and reduce dependency on glasses or contact lenses.
Corneal allogenic intrastromal ring segments (CAIRS)
 The latest advancement in corneal ring segment surgery is CAIRS, where donor corneal tissue is inserted instead of traditional synthetic implants. Because the CAIRS surgery uses biocompatible donor tissue, it minimises risks of rejection, scarring, and implant extrusion.
The latest advancement in corneal ring segment surgery is CAIRS, where donor corneal tissue is inserted instead of traditional synthetic implants. Because the CAIRS surgery uses biocompatible donor tissue, it minimises risks of rejection, scarring, and implant extrusion.
Performed in a day hospital using femtosecond laser technology, the CAIRS procedure involves creating precise corneal channels to insert ring-shaped donor tissue. Treatment can be customised for each patient’s unique corneal anatomy. As a minimally invasive keratoconus surgery, it allows for faster recovery, typically two to three days, and significant visual improvements within weeks. CAIRS is particularly beneficial for patients who cannot tolerate contact lenses or have experienced limited success with alternatives like corneal cross-linking or synthetic corneal implants.
Learn more about CAIRS here.
Corneal collagen cross-linking
Corneal cross-linking surgery can effectively stop the progress of keratoconus.2 It involves a combination of collagen and riboflavin (vitamin B2), which are activated by ultraviolet light to significantly strengthen the rigidity of the cornea.
The top layer of the cornea (epithelium) is often removed first using gentle debridement. The cornea is then saturated with collagen and riboflavin, and UV light applied to activate the solution. This causes the collagen strands to bond across the cornea and strengthen it. Early treatment with collagen cross-linking can slow or sometimes even stop the progression of keratoconus.
The procedure takes approximately one hour and is performed as an outpatient procedure in the clinic. Patients usually experience some mild discomfort in the immediate post-operative period.
Following treatment, the patient is fitted with a contact lens that stays in place for up to three days. Antibiotic drops are applied to the treated eye until the surface of the eye has healed. This is followed by steroid drops for approximately 5 to 6 weeks.
Corneal collagen cross-linking for keratoconus attracts a Medicare rebate. Contact your nearest Vision Eye Institute clinic for more information.
Corneal transplantation (keratoplasty)
This will only be suggested if all other keratoconus treatments options have been exhausted. About 10–20% of patients eventually require corneal transplantation.3
There are two types of corneal transplants – partial-thickness and full-thickness (or penetrating). It is usually the latter that is recommended for patients with keratoconus.
A corneal transplant is a complex procedure and requires admission to a day surgery. It is generally performed under local anaesthetic, with the option of a sedative. During the procedure, your surgeon will cut out the abnormal section of the cornea and replace it with donor cornea, which will be stitched into place. The stitches will be removed at a later date. Your own corneal cells will gradually grow and fuse to the donor tissue. Full recovery from this type of keratoconus surgery can take up to a year.
Future treatments
Corneal transplantation can be challenging to access due to the limited number of donor corneas available. However, Vision Eye Institute ophthalmologist Prof Gerard Sutton and his BIENCO consortium of experts from leading Australian institutions have developed world-first technology to bioengineer full-thickness corneas. This technology could remove the need to use corneal tissue from deceased donors.
Recently, BIENCO secured a $35 million grant from the Australian Government to move to its next phase of building a manufacturing and distribution facility in Sydney for bioengineered corneas. Read more about Prof Sutton’s research grant award and plans for the future of corneal transplantation here.
Clinic team
NSW
-

Prof Colin Chan
MBBS(Hons) MPhil FRANZCO
Locations
- Chatswood
Book a consultationwith Prof Colin ChanQLD
SA
VIC
-

Dr Uday Bhatt
MBBS DTMH DO MSc(EBP) FRCSEd FRCOphth FWCRS FRANZCO
Locations
- Camberwell
- Coburg
- Footscray
Book a consultationwith Dr Uday Bhatt
Dr Alex Ioannidis
MBBS FRCOphth FRANZCO
Locations
- Blackburn South
- Camberwell
- Coburg
Book a consultationwith Dr Alex IoannidisReferences
1. Keratoconus Australia. Contact lenses & spectacles [Internet]. Australia: Keratoconus Australia; [date unknown] [cited 2021 Jan 27]. Available from: https://www.keratoconus.org.au/treatments/contact-lenses/
2. Keratoconus Australia. Corneal crosslinking [Internet]. Australia: Keratoconus Australia; [date unknown] [cited 2021 Jan 27]. Available from: https://www.keratoconus.org.au/treatments/corneal-collagen-crosslinking/
3. Godefrooij et al. Nationwide reduction in the number of corneal transplantations for keratoconus following the implementation of cross-linking. Acta Ophthalmol. 2016 Nov;94(7):675-678. doi: 10.1111/aos.13095. Epub 2016 May 23. doi: 10.1111/aos.13095The information on this page is general in nature. All medical and surgical procedures have potential benefits and risks. Consult your ophthalmologist for specific medical advice.
Date last reviewed: 2026-04-08 | Date for next review: 2028-04-08






